

Legs bothering you? Well join the The White Noise Podcast as we pick the brain of Dr. Andy Berkowski, clinical associate professor and restless leg expert at the University of Michigan. Learn all about the diagnosis and management of restless legs syndrome. There is also a guest appearance by hepcidin, the bouncer at Club Ferritin.
CME credit link will be here when available
Show Notes – Season 1, Episode 4 – Restless legs syndrome
Time stamps
0:30 – Introduction
2:30 – Interview starts
7:40 – Picks of the month
12:50 – Case
13:50 – Initial thoughts on case
14:00 – Diagnosis of restless legs syndrome
16:50 – Diagnostic criteria for restless legs syndrome
17:40 – Difficulties in diagnosis
22:20 – Key questions to ask in taking history
24:00 – Periodic limbs vs restless legs syndrome
28:30 – Pathogenesis of restless legs syndrome
31:00 – History of Willis-Ekbom disease
35:50 – Case
36:40 – Medications for restless legs syndrome
38:30 – Dopamine agonists
43:30 – Alpha-2-delta-ligands
45:00 – Iron therapy
50:10 – PO vs IV iron supplementation
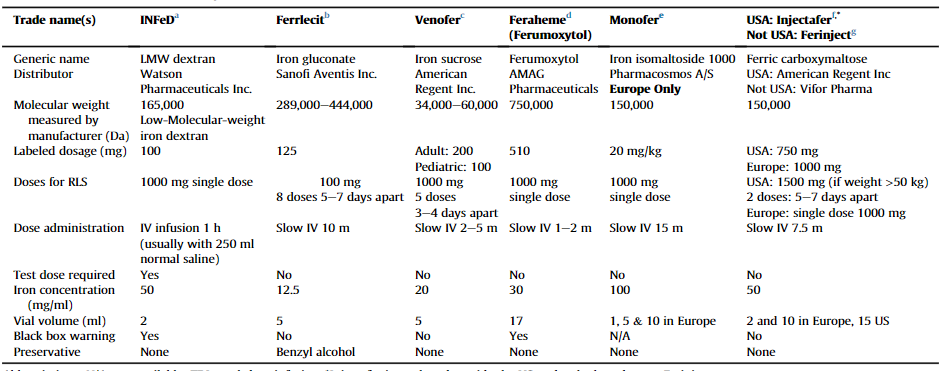
58:45 – IV iron formulations
1:00:30 – Narcotics
1:05:03 – Augmentation
1:09:00 – Non pharmacologic therapies
1:11:10 – Medications that worsen restless leg syndrome
1:16:00 – Screening for restless legs syndrome
1:18:00 – Follow-up of restless legs syndrome patients
1:18:50 – Sleep apnea and restless legs syndrome
1:20:10 – Take home points
1:22:00 – Interview end
Definitions
Augmentation: The process by which the symptoms of restless legs syndrome occur earlier in the day, become more severe, are less responsive to treatment, and spread to other parts of the body (e.g. arms and trunk), usually due to treatment with escalating doses of dopaminergic medications.
Restless legs syndrome: A condition characterized by an urge to move one’s legs (often accompanied by unpleasant sensations in the legs) that is most prominent at rest, partially or totally relieved by movement, and classically worse in the evening. The symptoms must not be better explained by another condition such as peripheral neuropathy.
Periodic limb movements of sleep: Periodic, repetitive, stereotyped limb movements that occur during sleep. American Academy of Sleep Medicine (AASM) scoring criteria require a minimum of 4 limb movements in series with 5-90 seconds between movements. Periodic limb movements of sleep are seen in the majority of patients with restless legs syndrome who undergo polysomnography.
Periodic limb movement disorder: A disorder characterized by more than 15 periodic limb movements per hour of sleep in adults (greater than 5 in children) that cause a significant sleep disturbance and/or functional impairment not better explained by a different disease entity.
Akathisia: An inner sense of restlessness and desire to move that is often caused by dopamine antagonist medications, is usually generalized (not limited to the legs), and is unlikely to be totally relieved by movement.
Clinical Pearls
- Restless legs is a clinical diagnosis
- The hallmark of the disease is a SENSATION of the need to move.
- There must be a circadian component to make a diagnosis.
- Augmentation will almost inevitably occur with dopamine agonists.
- Target ferritin >75 and transferrin saturation greater than 20% for iron repletion.
- Obtain fasting ferritin levels.
- Some times less iron is better than too much; if supplementing with daily PO iron and there is no improvement to ferritin levels consider cutting dose in half or switching to every other day dosing.
- Vitamin C supplementation increases iron absorption.
- Clinical practice is trending away from starting with dopamine agonists as first line agents.
- Making sure that iron is at adequate levels is the first step in management.
- Judicious use of opiates may be of benefit to the patient: This decision should be made after thorough risk benefit discussion with the patient.
- If patient has been stable on medication and RLS symptoms recur, check ferritin levels first.
Diagnosis of restless legs syndrome:
- Obtaining a thorough history the the cornerstone to making a correct diagnosis of restless leg syndrome. Things to elicit are whether the patient endorses a sensory component vs just a motor component.
- Diagnosis may be difficult when there are other co-morbid conditions such as peripheral neuropathy, or chronic pain. The sensory component and urge to move will help in distinguishing restless leg from other conditions.
- This is a clinical diagnosis; there are no tests that need to be done.
- International restless leg syndrome study group diagnostic criteria.
Treatment of restless legs syndrome:
- Treatment begins with checking ferritin and transferrin levels. Ferritin levels of less than <75 ng/ml, and/or transferrin saturation of less than 20% may indicate that iron supplementation is warranted.
- Typically PO iron supplementation is started, unless there is a contraindication to oral therapy (poor absorption, gastric bypass ect).
- Supplementation of PO iron with PO vitamin C is recommended; lower doses of iron may be more beneficial then higher doses.
- If IV supplementation is needed, see formulation list below. Newer formulations are safe, and the side effect profile is low.
- Sample iron supplementation algorithm
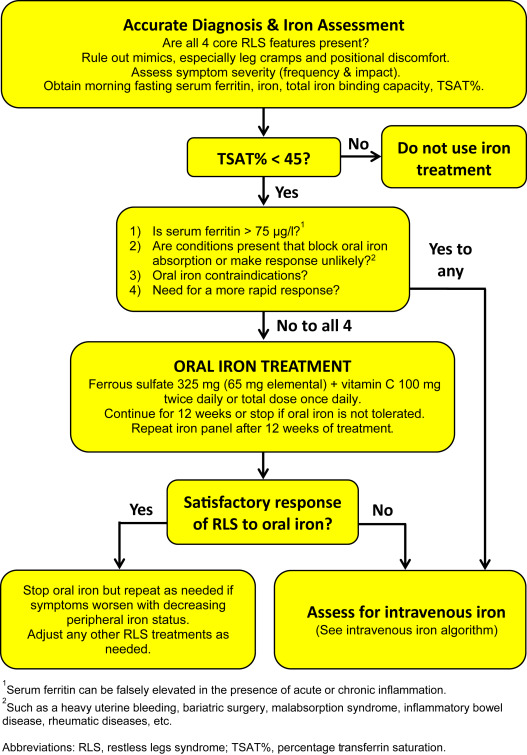
- If symptoms persist despite adequate supplementation of iron then initiation of therapy with an alpha-2-delta-ligand is recommended.
- Due to risks of augmentation dopamine agonists are not recommended, unless other forms of therapy are contraindicated.
Goals and objectives
Goals
Listeners of this episode will able to recognize restless legs syndrome in the clinic and be familiar with treatment strategies.
Objectives
After listening to this episode, listeners will be able to…
1. Recognize patients with restless legs syndrome disorder based on history.
2. Compare the different forms of iron supplementation, and formulate a therapeutic plan for the patient.
3. Describe the various treatments for restless legs syndrome.
4. Implement a treatment plan based on a patient’s specific needs.
5. Recognize patients undergoing augmentation, and formulate treatment plans.
6. Be familiar with the opioids used in management of restless legs syndrome.
7. Discuss the risks and benefits of different pharmacologic treatment options with the patient.
Dr. Berkowski’s Suggested reading list.
- “A 10-year, longitudinal assessment of dopamine agonists and methadone in the treatment of restless legs syndrome”
- “Comparison of Pregabalin with Pramipexole for Restless Legs Syndrome”
- “Clinical efficacy of ferric carboxymaltose treatment in patients with
restless legs syndrome” - White Paper on prevention and treatment of RLS by IRLSSG
- “Evidence-based and consensus clinical practice guidelines for the iron treatment of restless legs syndrome/Willis-Ekbom disease in adults and children: an IRLSSG task force report”
Patient resources
- Restless Legs Syndrome Foundation
- Restless Legs Syndrome, National Sleep Foundation
- Restless Legs Syndrome, American Thoracic Society Patient Education/Information Series
Picks of the month
Disclosures
The authors of The White Noise Podcast do not have any relevant financial disclosures.